
Dr Matthew A Butkus
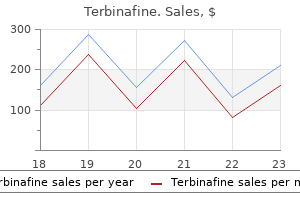
Terbinafine dosages: 250 mg
Terbinafine packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills

Tumor markers: Tumor markers are substances that can generally be discovered within the blood when a person has most cancers. Still, these exams can sometimes be helpful, together with other checks, in determining if somebody has most cancers. If all of the most cancers has been removed, these exams may additionally be accomplished to look for indicators the most cancers may be coming again. Percutaneous (through the skin) biopsy: For this check, a health care provider inserts a thin, hole needle through the skin over the stomach and into the pancreas to take away a small piece of a tumor. The doctor passes an endoscope (a skinny, flexible, tube with a small video digicam on the end) down the throat and into the small gut close to the pancreas. They may be helpful if the surgeon is worried the most cancers has unfold past the pancreas and desires to have a look at (and probably biopsy) different organs within the stomach. The most typical method to do a surgical biopsy is to use laparoscopy9 (sometimes known as keyhole surgery). The surgeon can look at the pancreas and different organs for tumors and take biopsy samples of abnormal areas. Instead, the physician will proceed with surgery, at which era the tumor cells may be looked at in the lab to affirm the prognosis. During surgery, if the doctor finds that the cancer has unfold too far to be removed fully, solely a sample of the cancer may be removed to affirm the diagnosis, and the the rest of the deliberate operation will be stopped. If treatment (such as chemotherapy or radiation) is planned earlier than surgery, a biopsy is required first to make sure of the analysis. This would possibly have an effect on whether certain focused remedy drugs10 might be useful as a part of remedy. Testing for these gene mutations can generally affect which treatments may be useful. It may additionally affect whether or not other relations should think about genetic counseling and testing as nicely. Cancers with similar phases tend to have a similar outlook and are often treated in much the identical means. It is predicated on the results of physical exam, biopsy, and imaging exams (see Tests for Pancreatic Cancer). Numbers or letters after T, N, and M present extra particulars about each of those factors. The cancer is rising outside the pancreas and into close by main blood vessels (T4). The most cancers has unfold to distant websites such because the liver, peritoneum (the lining of the stomach cavity), lungs or bones (M1). Tumor grade the grade describes how carefully the cancer appears like regular tissue under a microscope. Low-grade cancers (G1) tend to grow and spread more slowly than high-grade (G3) cancers. Most of the time, Grade three pancreas cancers are inclined to have a poor prognosis (outlook) compared to Grade 1 or 2 cancers. Borderline resectable this term is used to describe some cancers which may have just reached nearby blood vessels, but which the medical doctors really feel would possibly still be eliminated utterly with surgical procedure. Some type of surgery would possibly nonetheless be accomplished, but it will be a less extensive operation with the goal of preventing or relieving signs or issues like a blocked bile duct or intestinal tract, as an alternative of making an attempt to cure the most cancers. Surgery may nonetheless be carried out, however the objective can be to forestall or relieve symptoms, not to attempt to cure the cancer. International consensus on definition and standards of 19 American Cancer Society cancer. Last Revised: December 18, 2017 Survival Rates for Pancreatic Cancer Survival charges may give you an idea of what proportion of individuals with the same kind and stage of cancer are still alive a sure amount of time (usually 5 years) after they were diagnosed. Your doctor is acquainted with your scenario; ask how these numbers could apply to you.
The initial recommended dose of valproic acid is roughly 15 mg/kg/day in children or 400�500 mg/day in adults. This could be increased subsequently, as necessary and as tolerated, by 250�500 mg/day (or 5�10 mg/kg/day in children) at appropriate intervals. In genetic (idiopathic) generalized epilepsies, monotherapy with day by day doses between 10 and 20 mg/kg is often sufficient for full seizure control [20]. However, equally good outcomes have been achieved with a single daily dose, which may be defined by the pharmacodynamic profile of valproic acid. In truth, it seems that, no less than in some cases, the maximal therapeutic effect could lag by days and even weeks behind the achievement of steady doses or serum drug concentrations. As a result of animal research suggesting that teratogenicity may be associated to excessive peak serum valproic acid concentrations, it has been beneficial that in girls of childbearing potential extended launch formulations must be most well-liked to another treatment form [123]. This route can also be used for the treatment of standing epilepticus or where fast seizure control is required. In this case, the usual initial dose is 15�20 mg/kg administered over 5�10 min (at a price of 1. However, extra fast administration (up to 6 mg/kg/ min) of loading doses (up to 45 mg/kg) has been nicely tolerated [125]. A subsequent administration should be given inside 6 h in these receiving intravenous replacement therapy or bolus dosing, due to the rapid fall in serum drug concentrations and the attainable re-emergence of seizures. Likewise, extreme hepatotoxicity is unlikely to be detected by routine monitoring of liver enzymes, due to its fast onset and progression. Serum ammonia should be investigated in patients presenting with mental status changes, however should be interpreted with caution as elevated ranges are more likely to be discovered in lots of patients taking valproic acid. If gastrointestinal symptoms happen, particularly vomiting and abdominal ache, amylase and lipase ought to be checked, in addition to liver function exams. Valproate: a reappraisal of its pharmacodynamics properties and mechanisms of action. Bioavailability of sodium valproate suppositories throughout repeated administration at steady-state in epileptic children. Bioavailability of a divalproex extended-release formulation versus the conventional divalproex formulation in adult sufferers receiving enzyme-inducing antiepileptic medication. Comparison of sprinkle versus syrup formulations of valproate for bioavailability, tolerance, and preference. Variable free and whole valproic acid concentrations in sole- and multidrug therapy. Effects of age and antiepileptic drugs on protein binding and intrinsic clearance. Valproic acid efficacy, toxicity and pharmacokinetics in neonates with intractable seizures. Valproic acid: a reappraisal of its pharmacological properties and scientific efficacy in epilepsy. Clinical and pharmacokinetic observations on sodium valproate: a 5-year follow-up research in a hundred youngsters with epilepsy. Effect of felbamate on valproic acid disposition in healthy volunteers: inhibition of -oxidation. Conversion to lamotrigine monotherapy from valproate monotherapy in older adolescent patients with epilepsy. Comparative examine of ethosuximide and sodium valproate in the treatment of typical absence seizures (petit mal). Comparison of ethosuximide with sodium valproate as monotherapies of absence seizures. Ethosuximide, valproic acid, and lamotrigine in childhood absence epilepsy: Initial monotherapy outcomes at 12 months. [newline]The epilepsies: the analysis and management of the epilepsies in adults and kids in primary and secondary care. Phenobarbitone, phenytoin, or sodium valproate for newly recognized epilepsy: a randomized comparative monotherapy trial. A comparability of valproate with carbamazepine for the therapy of complex partial seizures and secondarily generalized tonic clonic seizures in adults. A multicentre comparative trial of sodium valproate and carbamazepine in adult onset epilepsy. Phenytoin versus valproate monotherapy for partial onset seizures and generalised onset tonic�clonic seizures.
A double-blind managed scientific trial of oxcarbazepine versus phenytoin in adults with beforehand untreated epilepsy. A double-blind controlled scientific trial of oxcarbazepine versus phenytoin in kids and adolescents with epilepsy. A double-blind controlled clinical trial: oxcarbazepine versus sodium valproate in adults with newly diagnosed epilepsy. Oxcarbazepine: double-blind randomized, placebo-controlled, monotherapy trial for partial seizures. Safety and efficacy of oxcarbazepine 1200 mg/day in patients with current onset partial epilepsy. Oxcarbazepine monotherapy for partial onset seizures: a multicenter, double-blind, clinical trial. Oxcarbazepine adjunctive therapy in infants and younger kids with partial seizures. Therapeutic experiences with 947 epileptic out-patients in oxcarbazepine treatment. Efficacy, tolerability, and side effects of oxcarbazepine monotherapy: a prospective research in adult and elderly sufferers with newly diagnosed partial epilepsy. Oxcarbazepine reduces seizure frequency in a excessive proportion of patients with each newly recognized and refractory partial seizures in medical apply. A multicenter trial of oxcarbazepine oral suspension in kids newly recognized with partial seizures: a medical and cognitive evaluation. Retention fee of oxcarbazepine monotherapy in an unselected population of grownup epileptics. Long-term safety and tolerability of oxcarbazepine in painful diabetic neuropathy. The effect of oxcarbazepine in peripheral neuropathic ache is dependent upon ache phenotype: a randomized, double-blind, placebo-controlled phenotype-stratified examine. A double-blind, randomized, placebo-controlled trial of oxcarbazepine within the therapy of bipolar dysfunction in children and adolescents. Neuroprotective results of anticonvulsants in rat hippocampal slice cultures uncovered to oxygen/glucose deprivation. Oxcarbazepine and atypical evolution of benign idiopathic focal epilepsy of childhood. Worsening of seizures by oxcarbazepine in juvenile idiopathic generalized epilepsies. Cognitive effects of oxcarbazepine and phenytoin monotherapy in newly recognized epilepsy: one year observe up. The cognitive effects of oxcarbazepine versus carbamazepine or valproate in newly diagnosed youngsters with partial seizures. Vitamin D ranges and bone turnover in epilepsy patients taking carbamazepine or oxcarbazepine. The effects of oxcarbazepine and valproate therapies on progress in children with epilepsy. Lipid profile and thyroid hormone concentrations in children with epilepsy handled with oxcarbazepine monotherapy: a prospective long-term study. The evaluation of thyroid capabilities, thyroid antibodies, and thyroid volumes in kids with epilepsy throughout shortterm administration of oxcarbazepine and valproate. Oxcarbazepine in the therapy of epilepsy in children and adolescents with mental incapacity. Improved quality of life in sufferers with partial seizures after conversion to oxcarbazepine monotherapy. Oxcarbazepine for remedy of partial epilepsy: a review and suggestions for clinical use. Prevention of early postoperative seizures in sufferers with main mind tumors: preliminary experience with oxcarbazepine. Multicentre observational study evaluating instant and progressive switching from carbamazepine to oxcarbazepine in patients with epilepsy. Relationship between serum mono-hydroxy-carbazepine concentrations and antagonistic results in sufferers with epilepsy on high-dose oxcarbazepine therapy. Temporal pattern of oxcarbazepine and phenytoin withdrawal seizures during epilepsy monitoring. Adjunctive treatment of main generalized tonic-clonic seizures in adults and children from 12 years of age with genetic (idiopathic) generalized epilepsy 2, 4, 6, eight, 10, 12 mg tablets Initially 2 mg, rising every 2 weeks or more in 2-mg steps.

The outcomes of 19 measures of cognitive skills and 18 measures of adjustment and mood showed solely findings attributable to chance. Long-term cognitive outcomes have been assessed in a double-blind, placebo-controlled, parallel-group, add-on study with an open-label extension involving 18- to 24-month follow-up [59]. The every day dosages within the long-term follow-up of this study had been larger than within the previous stories. In another add-on study, 41 patients with refractory epilepsy were randomly assigned to either tiagabine or topiramate treatment and obtained neuropsychological testing at baseline, after titration (3 months), and through the upkeep section (another three months). Consistent with different stories, topiramate but not tiagabine appeared to be associated with persistent negative cognitive side-effects on frontal lobe-associated features, the diploma of which may be estimated by the truth that this effect was observed with a really small pattern dimension [60]. Potential dose-related results of tiagabine on cognition and mood were studied in a conversion-to-monotherapy examine evaluating doses of 6 mg/day and 36 mg/day tiagabine as monotherapy in beforehand uncontrolled epilepsy sufferers [61]. In most preclinical and scientific studies, the tiagabine dose was expressed by way of milligrams of tiagabine hydrochloride. Initial dosages can be given twice a day, however a swap to 3 times every day dosing is recommended with dosages above 30�32 mg/day. Tiagabine should all the time be taken with meals, and preferably on the finish of meals, to keep away from fast rises in plasma concentrations. Individual dosing 4 times day by day may be helpful, no less than with larger doses. The ordinary higher limit of maintenance dosages is 50�56 mg/day in patients taking enzyme-inducing drugs and 30�32 mg/day in sufferers not taking enzyme-inducing medication. However, excessive daily doses of no less than 70�80 mg are well tolerated in some individual sufferers. Comparison of the preclinical anticonvulsant profiles of tiagabine, lamotrigine, gabapentin and vigabatrin. Protection towards dendrotoxin-induced clonic seizures in mice by anticonvulsant medicine. Effects of anticonvulsant medication on 4-aminopyridine-induced clonic seizures in mice. Tiagabine exerts an antiepileptogenic impact in amygdala kindling epileptogenesis within the rat. Tiagabine prevents seizures, neuronal injury and reminiscence impairment in experimental standing epilepticus. Vigabatrin and tiagabine are pharmacologically completely different medication: a preclinical research. Pharmacokinetics of tiagabine as add-on therapy in sufferers taking enzyme-inducing antiepilepsy drugs. Pharmacokinetics of tiagabine, a gamma-aminobutyric acid-uptake inhibitor, in healthy topics after single and a quantity of doses. Tiagabine: a evaluation of its pharmacodynamic and pharmacokinetic properties and therapeutic potential in the management of epilepsy. The pharmacokinetics of tiagabine in wholesome elderly volunteers and aged sufferers with epilepsy. A single-dose study to define tiagabine pharmacokinetics in pediatric sufferers with advanced partial seizures. Tiagabine adjunctive remedy in youngsters with refractory epilepsy: a single-blind dose escalating examine. Effects of renal impairment on the pharmacokinetics and tolerability of tiagabine. Pharmacokinetics and security of tiagabine in topics with various degrees of hepatic operate. Adjunctive treatment of partial seizures with tiagabine: a placebo-controlled trial. A double-blind, placebo-controlled trial of tiagabine given three-times every day as add-on therapy for refractory partial seizures. Tiagabine for advanced partial seizures: a randomised, add-on, dose-response trial.

Depth electrodes can carry four to 18 contacts along their size, normally spaced 5�10 mm apart at constant intervals. Depth electrodes are stereotactically inserted by the use of burr holes underneath native or basic anaesthesia (the latter method being most well-liked for longer procedures). The cortical surface is inspected through the burr holes to ensure the absence of superficial cortical vessels. A hole cannula is handed 1 cm from the target; a flexible electrode 1 cm longer than the cannula is then inserted, positioning the electrode on the precise target point. The introducer is then withdrawn while the wire electrode is steadily fed downward. The cable is fixed to the skin at the outlet by sutures or a burr gap button could additionally be used to safe the electrode cable following depth electrode placement. In the early Eighties, tomography and digital angiography had been used to find targets and choose an avascular aircraft to have the ability to implant the electrodes. This evolution has been driven by the advent of contemporary imaging strategies, stereotactic strategies and the use of robotic methods. More lately, there was a shift to frameless techniques with mechanical arms [41,42]. In some circumstances, especially auras and subclinical seizures, the ictal discharges could only be seen on depth electrode recordings [35,forty three,44]. However, it ought to be famous that mapping may also be achieved by way of a quantity of subdural strips albeit not perfect Subdural strips and grids can be used over any lateral neocortical floor, medial temporal structures in addition to the interhemispheric fissure and assist pattern intensive areas, especially when used at the aspect of depth electrodes Combined method (strips, grids and depths) depth electrode recordings (and verified by postsurgical outcome). Surgical problems In skilled palms, the morbidity of strip electrodes is small (1�3%) and normally associated with no long-term sequelae [33,47]. Infection is the most typical complication, and could be minimized by prophylactic antibiotics and by tunnelling the electrode wires to exit the skin a number of centimetres from the burr hole incision. Haemorrhagic problems are extremely rare, and cerebral oedema is uncommon with strip electrodes. The only major complications had been infections (two cases of meningitis and three superficial wound infections handled without squeal, and one mind abscess with permanent left hemiplegia). Common to both strategies Restricted sampling Increased sensitivity of intracranial electrodes comes at the price of restricted sampling. Subdural strip electrodes Inaccurate placement One of the principle limitations of subdural strip electrodes is the relative inaccuracy of the position methodology. Furthermore, placement could additionally be impeded by surgical adhesions related to prior events, thus deviating the strip from the intended target. Although the prevalence estimates are more likely to be conservative given selective reporting, they are often useful in counselling sufferers. The Yale group has famous delayed electrical seizure onset, initial electrical charge on the fringe of the grid and occasional problem in recording spontaneous ictal occasions [1]. Combining subdural strips and depth electrodes Depth electrodes Haemorrhage Early research reported a 1�4% danger of intracranial haemorrhage after depth electrode studies, accounting for more than half their major issues [34]. Meningitis is most typical, whereas intracerebral abscesses, scalp infections, cerebritis and subdural empyemas are much less commonly observed. To reduce their prevalence, some epilepsy centres will instigate prophylactic antibiotic protection from the time of depth electrode insertion till removal. Damage to brain parenchyma Since depth-electrode placement requires brain penetration, theoretical concerns have been raised about damage to the mind parenchyma. Pathological research have proven gliosis, cystic degeneration and microbial abscesses [35]. Signal abnormalities have been famous in 67% of sufferers, mostly consisting of punctate hyperintensities on long-repetition-time images in fifty seven patients who underwent stereotaxic placement of 210 depth electrodes [53]. Despite these findings, no vital deficits have but been noticed in the absence of subsequent problems or resective surgical procedure [54,55]. Epileptogenesis Animal research have instructed that depth electrode implantation alone may trigger epileptogenesis [56]. However, centres utilizing depth electrodes report similar short- and long-term success and relapse rates after resection as those not utilizing them [35]. Earlier research used the methodology developed by Talairach and Bancaud, and reported a morbidity rate of 1�5%, with intracerebral haemorrhage being the most common complication.

Colle du Japon (Agar). Terbinafine.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96124
Clinicians also can advocate that the patient seek a second opinion from another clinician to verify their impressions of an unsure diagnosis or if they imagine that this is able to be useful to the patient. Diagnostic consultations may additionally be arranged through the use of built-in practice models or diagnostic management groups (Govern, 2013; Porter, 2010; see Chapter 4). Kassirer concluded that: Absolute certainty in analysis is unattainable, irrespective of how much info we collect, how many observations we make, or how many tests we perform. As the inferential process unfolds, our confidence as [clinicians] in a given prognosis is enhanced by the gathering of knowledge that either favor it or argue in opposition to competing hypotheses. The choice to start therapy primarily based on a working diagnosis is informed by: (1) the diploma of certainty in regards to the analysis; (2) the harms and benefits of therapy; and (3) the harms and benefits of further informationgathering actions, together with the impact of delaying treatment. The dangers associated with diagnostic testing are essential considerations when conducting information-gathering actions in the diagnostic course of. While underuse of diagnostic testing has been a long-standing concern, overly aggressive diagnostic strategies have recently been acknowledged for his or her risks (Zhi et al. When considering diagnostic testing choices, the hurt from the procedure itself must be weighed in opposition to the potential data that might be gained. For some sufferers, the danger of invasive diagnostic testing may be inappropriate due to the chance of mortality or morbidity from the test itself (such as cardiac catheterization or invasive biopsies). In addition, the chance for hurt must bear in mind the cascade of diagnostic testing and remedy selections that could stem from a diagnostic check outcome. Included in these assessments are the potential for false positives and ambiguous or slightly irregular take a look at outcomes that lead to further diagnostic testing or pointless remedy. In addition, there are isolated instances where the morbidity and the mortality of a diagnostic procedure and the probability of disease is sufficiently excessive that vital remedy has been given empirically. Moroff and Pauker (1983) described a call analysis during which a 90-year-old training lawyer with a model new 1. Some diagnoses can be determined in a really quick time-frame, while months might elapse before different diagnoses could be made. This is partially because of the rising recognition of the variability and complexity of illness presentation. Similar signs may be related to numerous different diagnoses, and signs might evolve in numerous ways as a illness progresses; for example, a illness affecting a quantity of organs could initially contain symptoms or signs from a single organ. At the outset, it can be very difficult to decide which explicit prognosis is indicated by a selected combination of symptoms, especially if symptoms are nonspecific, such as fatigue. Diseases can also current atypically, with an uncommon and unexpected constellation of signs (Emmett, 1998). Adding to the complexity of the time-dependent nature of the diagnostic process are the numerous settings of care in which prognosis happens and the potential involvement of multiple settings of care inside a single diagnostic course of. Henriksen and Brady noted that this process-for sufferers, their households, and clinicians alike-can usually feel like "a disjointed Copyright � National Academy of Sciences. These embody diagnoses that can lead to significant patient harm if not acknowledged, recognized, and treated early, corresponding to anthrax, aortic dissection, and pulmonary embolism. Sometimes making a timely analysis depends on the quick recognition of symptoms outside of the health care setting. In these cases, the advantage of treating the disease promptly can greatly exceed the potential harm from pointless treatment. Consequently, the threshold for ordering diagnostic testing or for initiating treatment becomes quite low for such health issues (Pauker and Kassirer, 1975, 1980). In other circumstances, the potential hurt from quickly and unnecessarily treating a identified situation can result in a more conservative (or higher-threshold) approach within the diagnostic process. Diagnosis could be especially challenging in older sufferers because basic displays of disease are less frequent in older adults (Jarrett et al. Sensory limitations in older adults, such as listening to and vision impairments, can also contribute to challenges in making diagnoses (Campbell et al. Physical sicknesses often current with a change in cognitive standing in older individuals without dementia (Mouton et al. In older adults with mild to average dementia, such sicknesses can manifest with worsening cognition. There are indications that biases influence prognosis; one well-known instance is the differential referral of patients for cardiac catheterization by race and gender (Schulman et al.
A potential explanation might be its preferential affinity for different sodium channel subunits which have differential regional distribution within the brain [35]. The pharmacokinetics of lamotrigine in adults has beforehand been extensively reviewed [45,forty six,47,forty eight,49]. Absorption Lamotrigine is properly absorbed following oral administration and displays an absolute bioavailability of 98% in wholesome adult volunteers. After intake of the immediate-release formulation, peak concentrations occur at roughly 1�3 h after oral administration in adults [45,47,51], and 1�6 h in children [39,42]. A second peak or plateau might happen at 4�6 h post dose, which is probably a results of enterohepatic recycling of the drug [50]. Protein binding is unaffected by therapeutic concentrations of phenytoin, phenobarbital and valproic acid [47]. Studies in animals present that lamotrigine is broadly distributed in all tissues and organs, however little is thought of its differential tissue distribution in people. Measurement of lamotrigine concentrations in brain tissue obtained from resected mind tumours [53], and through autopsies [54], confirmed good penetration into the mind. Renal insufficiency Elimination Twelve volunteers with persistent renal failure (mean creatinine clearance 13 mL/min; vary 6�23 mL/min) and another six individuals present process haemodialysis had been every given a single 100-mg dose of lamotrigine [49]. Lamotrigine is metabolized by the liver, predominantly via N-glucuronidation, which is the rate-limiting step in lamotrigine elimination [45]. Approximately 70% of a single oral dose is recovered in the urine during the first 6 days and about 2% of an oral dose is excreted within the faeces. The apparent oral clearance of lamotrigine shows marked inter-individual variation and is considerably influenced by concomitant medicines and age [55]. Clearance is increased by 20� 170% in youngsters, but not for the first week of life. In comparative research of lamotrigine monotherapy, obvious oral clearance and quantity of distribution values were greater in children (0. In the research in youngsters, weight-normalized clearance appeared to be larger in kids youthful than 6 years (0. Age-related variations in lamotrigine clearance could probably be attributed to a relative reduction in liver measurement and hepatic blood flow in adolescents compared with younger kids [43,56]. Diminished glucuronidation of lamotrigine accounts for an age-related decline within the clearance of the drug within the aged [55]. Factors (other than age and co-medication) that affect lamotrigine pharmacokinetics Hepatic dysfunction the clearance of lamotrigine is reduced by about 25% in sufferers with mild hepatic dysfunction. A more distinguished discount in lamotrigine clearance is observed in patients with average and extreme hepatic impairment [49]. In sufferers with this syndrome, the clearance of lamotrigine clearance is reasonably lowered and the lamotrigine half-life is extended by about 35% compared with values present in wholesome subjects [58]. The adjustments in lamotrigine pharmacokinetics during pregnancy appear to be much less vital in women treated with a mixture of lamotrigine and valproic acid [63]. Lamotrigine is excreted in breast milk, which, along with the sluggish elimination of the drug in the infants, may result in `therapeutic concen- Co-administration of valproic acid, an inhibitor of lamotrigine glucuronidation, has been proven to markedly reduce lamotrigine clearance and to prolong markedly lamotrigine half-life [25]. Maximal inhibition of lamotrigine metabolism is already seen at a valproic acid dose of about 500 mg/day [71]. This can end result in pronounced peak�trough fluctuations in serum lamotrigine concentrations at steady state, particularly in kids underneath 6 years of age [47]. Dosing tips have been developed to optimize dose titration and target dosages in relation to age and kind of co-medication. For youngsters, these pointers include lower initiation doses and a slower titration to achieve concentrations near but not larger than those recommended for adults [56,74]. While some reports have instructed that lamotrigine clearance could also be accelerated by oxcarbazepine, a fastidiously performed research in wholesome volunteers found no proof of a pharmacokinetic interaction between these medicine [76]. On the opposite hand, an opposed pharmacodynamic interplay between lamotrigine and carbamazepine has been noticed.

Previously she served as president and chief government officer of the American Board of Internal Medicine. She is an adjunct professor of medicine and a senior fellow in the Department of Medical Ethics and Health Policy at the University of Pennsylvania School of Medicine, a former dean of medicine at Oregon Health and Science University, the chair of geriatrics at Mount Sinai School of Medicine in New York, and the chief of common inner medicine at the University of Chicago. Cassel is a prolific scholar, having authored and edited 14 books and greater than 200 revealed articles. Clancy, a basic internist and health services researcher, is a graduate of Boston College and the University of Massachusetts Medical School. Clancy holds an educational appointment at the George Washington University School of Medicine (clinical affiliate professor, Department of Medicine) and serves as a senior associate editor at Health Services Research. She is a member of the National Academy of Medicine and was elected a Master of the American College of Physicians in 2004. He has been a National Institutes of Health�funded investigator and has published extensively within the subject of prostate cancer and pathology. He is the recipient of a quantity of honors, including the Regents Award for Faculty Excellence on the University of Iowa and the Leonard Tow Humanism in Medicine Award. He was appointed the director of the new Critical Thinking Program at Dalhousie Medical School in 2012. In addition to his medical coaching, he holds a doctorate in experimental psychology and a fellowship in clinical psychology. His research is principally involved with clinical choice making, specifically on diagnostic error. He was on the organizing committee of the primary national convention on diagnostic error in 2008 and the second in 2009; he has contributed at every worldwide conference since. He has published greater than eighty journal articles and 30 guide chapters in the area of patient security, scientific decision making, and medical training reform. He was the senior editor on a major text, Patient Safety in Emergency Medicine (2009). Gallagher obtained his medical degree from Harvard University, completed his residency in Internal Medicine at Barnes Hospital, Washington University, St. Louis, and accomplished a fellowship within the Robert Wood Johnson Clinical Scholars Program, University of California, San Francisco. Gallagher has revealed more than ninety five articles and e-book chapters on patient safety and Copyright � National Academy of Sciences. His work in error disclosure obtained the 2004 Best Published Research Paper of the Year award from the Society of General Internal Medicine, in addition to the 2012 Medically Induced Trauma Support Services Hope Award. He also acquired a Robert Wood Johnson Foundation Investigator Award in Health Policy Research. He is senior creator of Talking with Patients and Families About Medical Errors: A Guide for Education and Practice, published in 2011 by the Johns Hopkins University Press. He is an appointed Commissioner on the National Commission on Physician Payment Reform. Gallagher is an lively member of many skilled organizations, including the American College of Physicians (Fellow), the Society for General Internal Medicine, and the American Society of Bioethics and Humanities. She is a Fellow of the American Academy of Nursing, a National Baldrige Examiner, and associate faculty within the Johns Hopkins Bloomberg School of Public Health, where she teaches a required course within the Master of Hospital Administration program. Formerly the director of strategic research initiatives at the Johns Hopkins Armstrong Institute, Dr. Goeschel serves on the board of the Maryland Patient Safety Center and is the creator of a number of guide chapters and greater than 65 peer-reviewed articles on subjects starting from implementation of large-scale clinical enchancment tasks to leadership for advancing the science of well being care supply and creating a tradition of accountability in well being care. Previous experience includes responsibility for high quality, risk administration, and service excellence in a Midwest instructing hospital and serving as an advisor to the World Health Organization Patient Safety Program. She is more and more involved in the study of diagnostic errors-both their etiology and understanding the connection of diagnostic error with preventable morbidity, mortality, and prices of care. He retired because the chief of medication on the Northport Veterans Affairs Medical Center in 2011. Graber has an in depth background in biomedical and health services analysis, with greater than eighty peer-reviewed publications. He is a national leader within the subject of affected person safety and originated Patient Safety Awareness Week in 2002, an event now acknowledged internationally. Graber has also been a pioneer in efforts to address diagnostic errors in medicine. In 2008 he convened and chaired the Diagnostic Error in Medicine convention sequence, and in 2011 he based the Society to Improve Diagnosis in Medicine ( In 2014 he grew to become the founding editor of a new journal, Diagnosis, dedicated to enhancing the quality and security of diagnosis, and he obtained the John M.
References
Desarrolló: Grupo Guadalupe S.R.L.